The latest real-world data are published, providing real evidence of the effectiveness of azelvudine in patients with COVID-19.
With the adjustment of preventive and control measures such as "Category B" and further global research on novel coronavirus infection (COVID-19), several anti-COVID-19 drugs have been urgently licensed in China, including Azivudine, the first small molecule oral anti-COVID-19 drug in China.
According to relevant studies, Azivudine can accelerate the clearance of virus and shorten the time to nucleic acid conversion in patients with moderate to mild COVID-19, and shorten the time to clinical symptoms of neocoronavirus infection in patients with moderate COVID-19. However, whether azelvudine reduces adverse clinical outcomes in hospitalised patients with COVID-19 is of particular concern to clinicians. This newly published real-world data confirms the true efficacy of Azulfidine in the clinic from a real-world perspective!
Real-world data confirming the clinical efficacy of Azulfidine!
- Study design
The study is a retrospective cohort study designed to assess the impact of azelvudine administration on clinical outcomes, including composite clinical progression and all-cause mortality. The analysis of the study focused on its effectiveness in patients admitted to hospital with COVID-19 who did not require any oxygen therapy initially.
Data were collected on 1505 consecutive patients with COVID-19 diagnosed at Xiangya Hospital, with a follow-up period of up to 29 days. A total of 452 adult inpatients were enrolled, with 226 patients in each of the 1:1 matched Azulfidine and control groups. Due to a shortage of medical resources and medication availability during the pandemic, the mean time from symptom onset to hospitalisation was 8.2 days, with only 12% of patients receiving azelvudine within 5 days of symptom onset. Patients were observed from the date of admission to the date of the outcome event, the date of discharge or the date of death, whichever came first.
- Study results
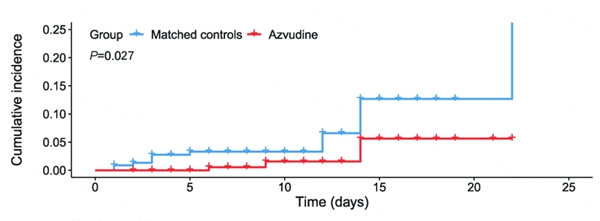
The incidence of the composite disease progression outcome was 4.21 per 1000 person-days (3.54%) in patients treated with Azivudine compared to 10.39 per 1000 person-days (7.52%) in the control group (Figure 1). All-cause mortality was 1.57/1000 person-days (1.33%) in patients treated with Azivudine compared to 6.00/1000 person-days (4.42%) in the control group (p=0.027) (Figure 2).
Cox regression analysis showed that azelvudine was associated with a significantly lower risk of combined disease progression (HR: 0.43; 95% CI: 0.18-0.99) and all-cause mortality (HR: 0.26; 95% CI: 0.07-0.94) in patients. Azulfidine significantly reduced the risk of composite disease progression by 57% and all-cause mortality by 74% in patients hospitalized with COVID-19.
2023020220571789.001.png
Figure 1 Combined clinical outcomes in the azelvudine group versus the control group
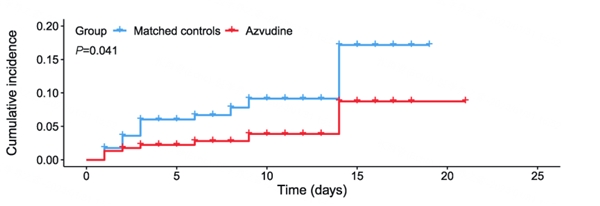
Figure 2 Incidence of all-cause mortality in the Azulfidine group versus the control group
In addition, the incidence of invasive mechanical ventilation between the two groups was also statistically significant according to the log-Rank test (p=0.020).
Taken together, the results of this real-world data suggest that azelvudine reduces the risk of disease progression and all-cause mortality in patients hospitalised with COVID-19.
New data fills a real-world gap as efficacy is confirmed by multiple sources!
As a broad-spectrum RNA virus inhibitor, Azivudine inhibits the RNA-dependent RNA polymerase (RdRp) of SARS-CoV-2, which is embedded in the viral RNA during synthesis, blocking RNA elongation and terminating RNA strand synthesis and viral replication. Since Azulfidine is enriched in the thymus and peripheral blood lymphocytes, it significantly reduces the viral load in the thymus, thereby enhancing the immune function of the body to suppress the new coronavirus. Thus, Azivudine, as a broad-spectrum RNA virus inhibitor, can play a role in both antiviral replication and immune protection.
A series of global multicentre randomised, double-blind, placebo-controlled Phase III clinical studies have been conducted with Azivudine tablets. The results of the Phase III Chinese study of Azivudine showed that subjects with log values ≥3 and log values ≥4 had a statistically significant greater reduction in viral load from baseline than the control group on day 5 of Azivudine. The results of the study in patients with moderate COVID-19 also showed that 36.31% of subjects showed clinical improvement after 7 days of azelvadine, which was clinically superior compared to the control group, and the median time to clinical improvement was significantly shorter in the azelvadine group (p<0.001).
In this published real-world study, the incidence of all-cause mortality was 1.33% in the azelvudine recipients compared to 4.42% in the control group, with a combined outcome rate of 3.54% and 7.52% in the two groups, respectively. The results, which are consistent with previous clinical studies, further reflect the effectiveness of azelvudine in real clinical practice and provide realistic evidence for its use in patients with COVID-19.
Based on the solid data, azelvudine has been recommended in several consensus guidelines or treatment protocols in the past, with an emphasis on early use:
- The 10th edition of the Novel Coronavirus Pneumonia Protocol recommends azelvudine for the treatment of medium-sized patients with COVID-19;
- The "Reference protocol for the treatment of new coronavirus pneumonia in the Department of Respiratory and Critical Care Medicine, Peking Union Medical College Hospital (December 2022 edition)" recommends the use of azelvudine in patients with relatively early disease duration and positive nucleic acid;
- The Expert Consensus on the Antiviral Treatment of Patients with Novel Coronavirus Infection (published on 12 January) emphasizes the early use of oral neo-coronaviruses, noting that it can be recommended in medium-sized infected and homebound patients with positive antigen or nucleic acid tests and high risk factors for disease progression (e.g. hypertension, diabetes, coronary artery disease, chronic obstructive pulmonary disease);
- In critically ill patients, azelvudine has also been recommended in the "Treatment Protocol for Novel Coronavirus Infections in Critical Care (Trial Version 4)" and its early use is recommended;
- The Hubei Provincial Guidelines for Primary Care recommends that Azulfidine tablets be given orally at 5mg daily on an empty stomach for those with a disease duration of less than 7 days or who are nucleic acid positive for new coronavirus, if Azulfidine tablets are available;
- The Guidelines for Primary Care and Services for Novel Coronavirus Infections (First Edition) recommends Azulfidine for the treatment of adult medium-sized patients with COVID-19; it may be recommended for patients with significant symptoms and pulmonary signs and positive antigen or nucleic acid tests for novel coronavirus infection if primary care facilities are not equipped to perform imaging;
Summary
Although the current epidemic strains have significantly reduced the rate of severe disease compared to the original strains, we should not be complacent. The availability of real-world data confirming the association of azelvudine treatment with composite disease progression outcomes and all-cause mortality risk in COVID-19 patients in the real world further strengthens clinical confidence in the use of azelvudine as a "weapon". We look forward to more real-world data on Azivudine in the future!